Malignant Mesothelioma Cancer
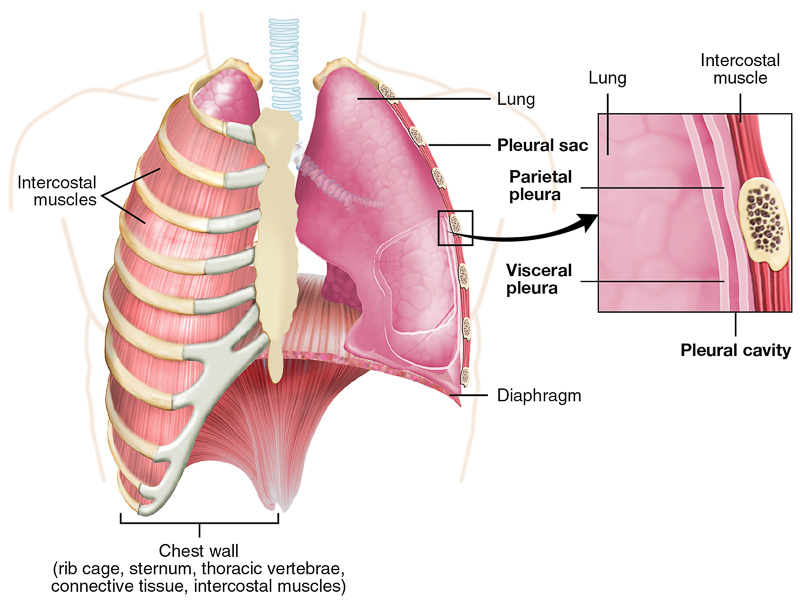
Mesothelioma may be a cancer of the mesothelium, a membrane that lines the within of the body's cavities, like the abdomen or chest. Three out of every four cases of mesothelioma disease begin within the chest cavity. Mesothelioma also can begin within the abdominal cavity and around the heart. Regardless of where they originate, malignant cells from the mesothelium can invade and damage nearby tissues. Cancer cells can also metastasize, or spread, to other parts of the body. Often by the time mesothelioma is diagnosed, the disease is advanced. The 5-year survival rate is around 5% to 10%. Most patients with mesothelioma of the lung die as a result of respiratory failure or pneumonia. Some patients get a small-bowel obstruction when the tumor extends through the diaphragm, a muscle that separates the chest and abdominal cavity. A smaller number of individuals die of complications of the heart when the tumor invades the pericardium -- a thin sac that surrounds the heart -- and therefore the heart itself.
Causes of Mesothelioma
The main risk factor for mesothelioma is working with asbestos. Asbestos may be a group of minerals with thin microscopic fibers. Because these fibers are resistant to heat, fire, and chemicals and don't conduct electricity, asbestos has been mined and used widely within the construction, automotive, and other industries. If tiny asbestos fibers are released into the air, as they're within the manufacturing process, they will be inhaled or swallowed, resulting in serious health problems. As many as 75% of mesothelioma cases are often linked to exposure to asbestos at work. There’s also some evidence that family members and others living with asbestos workers have an increased risk of developing mesothelioma, and possibly other asbestos-related diseases. This risk could also be the result of exposure to asbestos dust brought home on the clothing and hair of asbestos workers. Cases of mesothelioma have also been seen in people living close to asbestos mines. However, mesothelioma has been reported in some individuals with none knew asbestos exposure. Other, uncommon, but possible causes include: Zeolites. These minerals are chemically associated with asbestos. One of these related minerals, erionite, is common within the soil in some areas of Turkey, consistent with the American Cancer Society. Exposure to erionite is believed to be liable for high rates of mesothelioma rates in those areas.
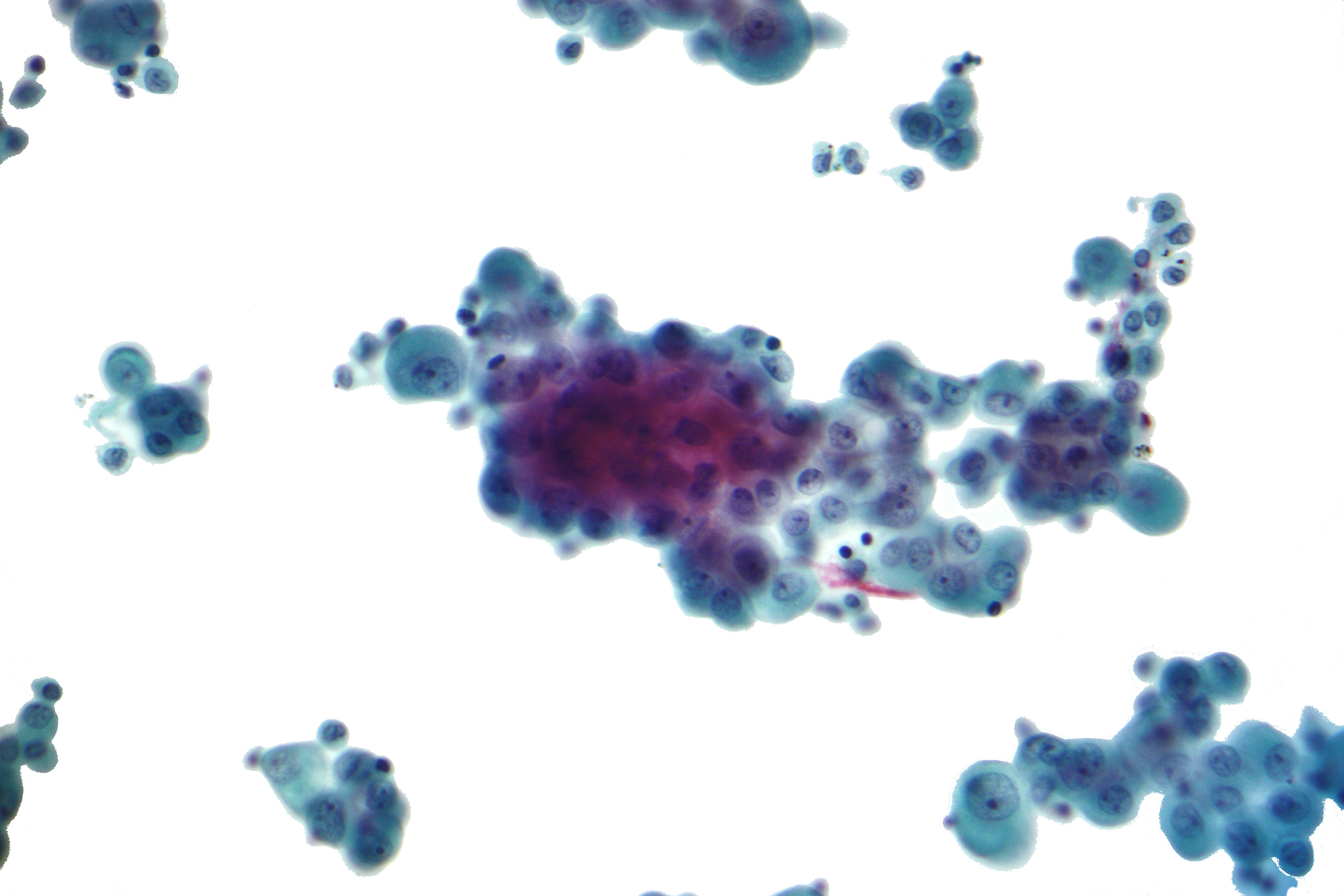
Diagnosis
There is no specific imaging modality that's diagnostic for MPM. However, the widely accepted first-line modality is computed tomography (CT) scan, which is usually one of the first imaging studies obtained when a patient presents with abdominal pain and distension. The use of further imaging is rarely needed for staging unless clinically indicated, as the extra-abdominal spread is rare. On CT, MPM appears as a solid, heterogeneous, soft tissue mass with irregular margins that enhances with the use of intravenous (IV) contrast. MPM tends to be more expansive than infiltrative so diffuse distribution throughout the abdominal cavity should raise suspicion. the shortage of a primary site with neither lymph node involvement nor distant metastases helps differentiate MPM from other intra-abdominal malignancies. Ascites is found in 60–100% of patients that are newly diagnosed. Other findings include caking, thickening or masses within the omentum, mesenteric nodules, peritoneal thickening, diaphragmatic involvement, scalloping of the intraabdominal organs like the liver and spleen, and loculated ascites. Some studies demonstrate that diffusion-weighted and dynamic gadolinium-enhanced MRI can more accurately estimate the disease burden of peritoneal disease, including MPM, but the usefulness for diagnostic purposes isn't well defined. Similarly, PET and PET/CT are evolving imaging modalities that are being used more frequently within the staging of cancers, but their value in evaluating and staging MPM is still unclear. based on cross-sectional imaging, the differential diagnosis for MPM can include peritoneal carcinomatosis, serous peritoneal carcinoma, ovarian carcinoma, lymphomatosis, and tuberculous peritonitis. Despite advances in imaging, there's ultimately no imaging finding that's specific for MPM. Serum chemistry and markers have limited utility for diagnostic purposes in MPM. Most of the research on serum markers has been done in pleural mesothelioma, with some patients shown to have elevations in CA-125, alpha-fetoprotein, CEA, mesothelin, osteopontin, and fibulin-3. Unfortunately, their sensitivities are too low to be used for diagnostic purposes. Levels of serum mesothelin-related protein (SRMP) have shown more promise, with a sensitivity of 60%. While not useful for diagnostic purposes in MPM, CA-125 and mesothelin have some promise as a marker of tumor response or surveillance. If initially elevated, serum CA-125 often normalizes to baseline levels after treatment and has been shown to correlate with post-treatment disease progression.
Mesothelioma Symptoms
Symptoms of mesothelioma appear when tumors spread, grow and press against the chest wall and therefore the abdominal cavity. chest pain and shortness of breath are the most common symptoms.
COMMON MESOTHELIOMA SYMPTOMS
- Dry coughing
- Shortness of breath
- Respiratory complications
- Pain within the chest or abdomen
- Fever or night sweats
- Pleural effusion (fluid around the lungs)
- Fatigue
- Weakness within the muscles
Staging
Staging MPM is difficult due to limitations in current imaging techniques, specifically within the accurate assessment of tumor size and nodal involvement. Surgical thoracoscopy, with additional mediastinoscopy to assess suspected nodal disease, is superior to computed tomography (CT) and is that the current gold standard for staging in MPM. However, not all patients are suitable to undergo this procedure, and thus image-based staging, whilst imperfect, is used for several MPM cases. There are a variety of staging classifications for MPM, all of which have limitations to be used in routine clinical practice. The consensus is that a tumor, node, metastasis-based system, using surgical information where available and radiology in its absence, should be employed to determine prognostic outlook altogether patients with MPM. One such system is that the International Mesothelioma interest group staging classification.